|
Back to 2014 Annual Meeting Abstracts
Nonoperative Management of Symptomatic Cholelithiasis in Pregnancy Is Associated With Frequent Antepartum and Early Postpartum Hospitalizations
April Jorge*1, Andrew J. Gawron1, Annapoorani Veerappan1, Nathaniel J. Soper2, Rajesh N. Keswani1
1Medicine, Northwestern University, Chicago, IL; 2Surgery, Northwestern University, Chicago, IL
Introduction:
Symptomatic gallstone disease during pregnancy is a leading cause of non-obstetric hospitalizations and operations. Although laparoscopic cholecystectomy (LC) is safe and efficacious in pregnancy (SAGES Guidelines, 2011), practice patterns are variable with nonoperative management favored by some providers. The aim of this study was to evaluate practice patterns and outcomes of pregnant patients undergoing nonoperative management for symptomatic cholelithiasis (SC).
Methods:
We performed a retrospective analysis of all patients who presented to a tertiary care academic center over a 42-month period (Jan 2009-July 2012). Women (age 18 or older) with uncomplicated SC during pregnancy (without cholecystitis, pancreatitis, choledocholithiasis, or cholangitis) were included. Patients were identified by querying an electronic data repository for relevant diagnoses, imaging, and procedure codes. Patients were also contacted via a standardized telephone survey to supplement the chart review and account for outside hospitalizations and treatments.
Results:
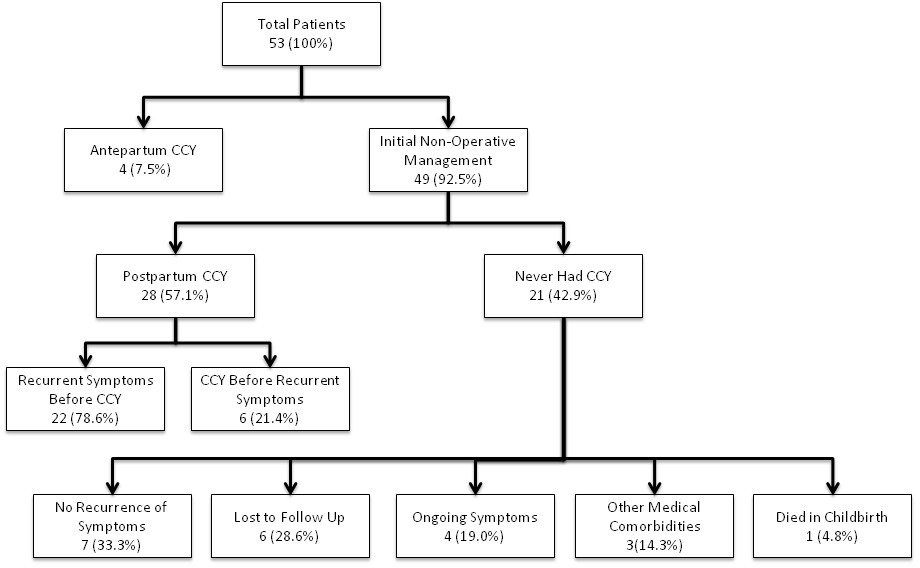
A total of 53 women (mean age 32.4y, SD 6.7) with SC were identified during the study period (Table 1). Mean gestational age at initial presentation was 23 weeks (9 patients in first, 22 in second, and 22 in third trimester). Four women (7.5%) underwent LC in the antepartum period, all in the second trimester (Figure 1). There were no maternal or fetal complications associated with LC.
Forty-nine women (92.5%) had initial non-operative management. Of these women, 18 (36.7%) were hospitalized more than once in the antepartum period (range 0-5 hospitalizations). Postpartum LC was performed in 28 women (57.1%), the majority (n=21) within 3 months postpartum. Of women who underwent postpartum LC, 22 (78.6%) had recurrent symptoms postpartum prior to LC, and 14 (50.0%) were readmitted at least once (median 1, range 1-4) postpartum for SC prior to undergoing LC.
In the remaining 21 women who never underwent LC (42.9%), long-term follow-up information was available in 15 (six could not be reached for telephone survey). Seven elected to not undergo LC due to absence of postpartum symptoms. Four patients had ongoing symptoms but had not undergone LC (one due to recurrent pregnancy). A single patient died from postpartum bleeding complications. Three women had other co-morbid medical conditions, and a decision to defer surgery was made in the postpartum period in conjunction with their providers.
Conclusions:
A minority of pregnant patients with SC undergo antepartum LC. In the remaining patients, many have multiple antepartum admissions for SC. Furthermore, in those who undergo LC, half do so only after postpartum admission for SC. Given the safety of antepartum LC, early surgical intervention during pregnancy may be the optimal strategy to reduce antepartum and early postpartum admissions.
Table 1. Overall Patient Demographics (n=53)
| Maternal Age at Symptom Onset, years (SD) | 32.4 (6.7) | | Gestational Age in weeks at Initial Presentation, mean (SD) | 23 (10.5) | | Maternal Gravidity, median (Range) | 2 (1-7) | | Third Trimester Symptom Onset | 22 (41.5%) | | Public Aid/Self-Pay | 21 (39.6%) | | Ethnicity | | | Caucasian (Non-Hispanic) | 18 (34.0%) | | Hispanic/Latino | 16 (30.1%) | | African American | 8 (15.1 %) | | Other/Declined Race | 11 (20.8%) |
 Figure 1. Flow chart depicting the clinical and surgical outcomes of 53 patients with symptomatic cholelithiasis over a 3.5 year period.
Back to 2014 Annual Meeting Abstracts
|