|
|
Back to 2014 Annual Meeting Abstracts
Persistent Functional Deficits and Symptoms Among Long-Term Survivors of Colorectal Cancer Treated With Surgery and Multimodality Therapy: Differences by Age At Initial Diagnosis
Christina Bailey*, Hop S. Tran Cao, Chung-Yuan Hu, George J. Chang, Barry W. Feig, Miguel Rodriguez-Bigas, Sa Nguyen, John M. Skibber, Y. Nancy You
Surgical Oncology, University of Texas, MD Anderson Cancer, Houston, TX
Background: Colorectal cancer (CRC) survival outcomes have significantly improved and increasing attention is now being turned to the needs of cancer survivors. We investigated the functional outcomes and symptoms reported by long-term (10 years) CRC survivors who underwent surgery and other multimodality treatments, and examined the key determinants of these outcomes.
Methods: A total of 1,215 eligible long-term CRC survivors were identified from an Institutional Tumor Registry. 415 survivors who had been diagnosed during young adulthood (Y, age 18-50 years) were matched at a 1:2 ratio to 801 patients diagnosed during later adulthood (L, age > 50 years), for tumor site (colon vs. rectum) and oncologic treatments received (surgical and nonsurgical). A cross-sectional survey study was conducted using the validated EORTC CRC module (CR29) including 4 functional scales and13 symptom scales. Scores were standardized by linear transformation (score range: 0-100) and were compared between Y and L patients using Student's t-test. Multivariate linear regression was performed to assess the impact of patient and treatment factors on functional outcomes.
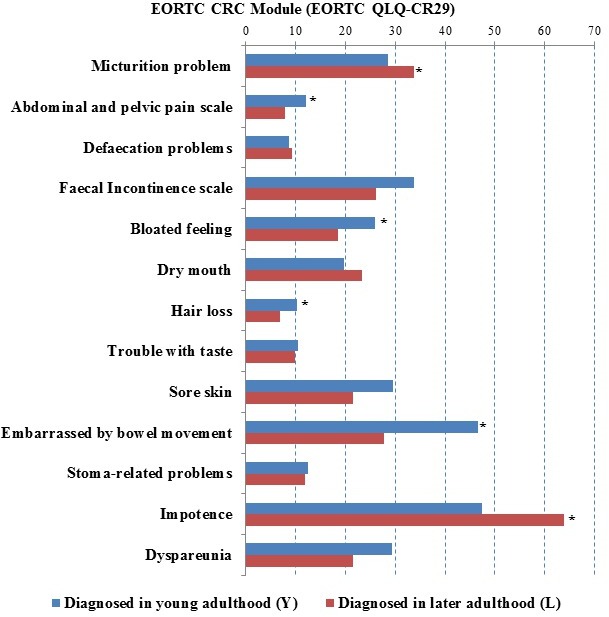
Results: 830 survivors responded at an interval of 10.8±3 years from diagnosis, including 282 Y patients (mean age at diagnosis 43±6 years) and 548 L patients (mean age at diagnosis 63±8 years). The response rate was 68% overall and in both subgroups. Subgroups did not differ in regards to tumor site (proximal colon, distal colon, rectum; p=0.592), radiation (p=0.538), surgical procedure (segmental colectomy, proctectomy without stoma, proctecomy with stoma, other; p=0.214) or presence of stoma (p=0.607), although chemotherapy was received by more Y patients (86.1 vs. 77.7%; p=0.004). Functional differences were identified, with Y patients reporting more anxiety (57.1 vs 69.6, p<0.001), worse body image perception (73.9 vs 81.8, p<0.001), better male sexual function (44.2 vs 55.7, p=0.002) and better female sexual function (68.1 vs 76.0, p=0.014) when compared to L patients. Among the 13 symptoms assessed, abdominal/pelvic pain, bloating, hair loss, and embarrassment with bowel movements were more significant among Y patients, while L patients reported more problems with micturition and impotence (Figure). After adjusting for patient and treatment factors, younger initial age at CRC diagnosis was the most influential independent contributor for more anxiety, while the presence of an ostomy had the strongest negative impact on body image.
Conclusion: Long-term survivors of CRC face ongoing deficits in function and symptoms. The initial age at CRC diagnosis impacted patient-reported experiences and may be associated with long-term coping. These persisting effects should inform the care of CRC patients and survivors.
Figure. Results of EORTC CRC module (EORTC QLQ-CR 29) symptom scales: a higher score indicates a higher level of symptomatology.
Back to 2014 Annual Meeting Abstracts
|