
|
|
Back to Annual Meeting Posters
Sarcopenia: Significant Independent Risk Factor for Poor Survival Following Esophageal Resection
Aaron S. Rickles*2, James C. Iannuzzi2, Dylan R. Nieman1, Michal J. Lada1, Kristin N. Kelly2, Fergal Fleming2, Jeffrey H. Peters1, John R. Monson2
1Surgery, University of Rochester, Rochester, NY; 2Department of Surgery, Surgical Health Outcomes & Research Enterprise, University of Rochester, Rochester, NY
Purpose:
Sarcopenia has been linked to poor survival in several types of cancer including breast, pancreatic, and colorectal. This study examines the effect of sarcopenia on survival outcomes after esophagectomy for cancer.
Methods:
A retrospective chart review was performed on patients who underwent esophageal resection between 2005-2012. Pre-operative CT imaging was used to measure total body fat, abdominal fat, and muscle mass. Muscle mass area at the level of the third lumbar vertebrae (psoas, erector spinae, and abdominal muscles) was normalized for patient height and sarcopenia was defined by sex-specific values as previously described (38.5 cm2/m2 for females, and 52.4 cm2/m2 for males). Data was collected on patient, tumor, and treatment characteristics. Kaplan-Meier survival curves and Cox Proportional Hazards were used to analyze the primary endpoint of overall survival over 5 years.
Results:
Out of 271 esophageal resections, 131 cases had CT scans available for analysis, of which 53 patients died over a median follow-up of 22 months. 32.1% (n=42) of patients met criteria for sarcopenia and on average sarcopenic patients were older (67 yo. vs. 61 yo., p=0.002), had less total fat (4168 cm3 vs. 4963 cm3, p=0.033) and less abdominal fat (1524 cm3 vs. 1876 cm3, p=0.043), however there was no statistically significant difference in waist circumference or body mass index between the two groups. There was also no difference between sarcopenic and non-sarcopenic groups based on gender, smoking status, comorbidities, presentation, tumor stage, resection margin status, number of locoregional lymph node metastases, leak rates, length of hospital stay, and use of neoadjuvant or adjuvant therapy. On Kaplan-Meier analysis sarcopenic patients had significantly worse overall survival compared to patients with normal muscle mass (log rank=0.012, Figure 1). 5-year overall survival was 62% for patients with normal muscle mass and 33% for patients with sarcopenia. After adjusting for differences in patient age and body fat composition in cox-proportional survival analysis, patients with sarcopenia had twice the risk of death over five years as compared to patients with normal muscle mass [HR=2.00; 95%CI=(1.13,3.56), p=0.018].
Conclusion:
Sarcopenia predicts worse overall survival after esophagectomy for cancer. While sarcopenia itself offers substantial prognostic value, these findings underscore the importance of optimizing patient nutrition and exercise status as part of the comprehensive cancer care to improve survival in this vulnerable population.
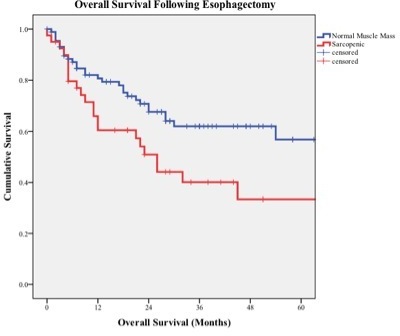
Figure 1. Kaplan-Meier analysis of overall survival for sarcopenic (red) and non-sarcopenic (blue) patients following esophageal resection for cancer (Log Rank Test = 0.012).
Back to Annual Meeting Posters
|

