|


|
Back to Annual Meeting Posters Endoscopic Ultrasound Staging of Stenotic Esophageal Cancers May Be Unnecessary to Determine the Need for Neoadjuvant Therapy Stephanie G. Worrell*, Daniel S. OH, Christina L. Greene, Steven R. Demeester, Jeffrey a. Hagen Keck School of Medicine of Univeristy of Southern California, Los Angeles, CA
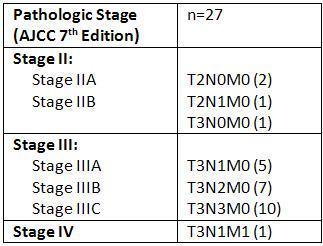
Introduction: Endoscopic ultrasound (EUS) is an essential component of pre-operative staging for esophageal cancer. EUS is used to determine which patients should have primary endoscopic or surgical therapy and which should have neoadjuvant therapy prior to resection. However, when the EUS endoscope cannot traverse a tumor, the role of pre-dilatation is controversial. Esophageal dilation of malignant strictures is associated with potential complications including perforation in 15% of cases. The aim of this study was to determine the pathologic stage of esophageal cancer treated by primary surgery without induction therapy when the EUS endoscope could not pass. We hypothesized that when the EUS endoscope cannot traverse the tumor, locally advanced disease (stage III) is present, and these patients should proceed to neoadjuvant therapy without the need for pre-dilatation and EUS staging. Back to Annual Meeting Posters
|
|||||||
© 2026 Society for Surgery of the Alimentary Tract. All Rights Reserved. Read the Privacy Policy.