|
Back to Annual Meeting Program
Surgery for Gallbladder Cancer in the US: Greater Need for Radical Cholecystectomy and Maximal Lymph Node Clearance
Thuy B. Tran*, Vijay G. Menon, Nicholas N. Nissen
Cedars-Sinai Medical Center, Los Angeles, CA
Background: Gallbladder cancer (GBC) is an uncommon cancer with poor overall survival and frequent local and metastatic relapse. GBC is often identified incidentally after cholecystectomy, in which case reoperation with portal lymph node dissection (LND) is frequently performed. The value of LND both for its staging and therapeutic value continues to be debated. In particular, the optimal extent of lymph node clearance is unclear.
Methods: The Surveillance, Epidemiology, and End Results (SEER) database was queried for patients diagnosed with GBC. Overall survival was analyzed using the Kaplan-Meier method and compared using Log rank testing. Cox proportional hazard modeling was used in multivariate analysis to identify predictors of survival using age, type of surgery (simple vs radical cholecystectomy), adjuvant treatment, stage, and number of lymph nodes examined. In addition, the contribution to survival of minimal LND (min-LND; 1-3 LN removed) vs maximal LND (max-LND; >3 LN removed) was evaluated separately within each of tumor Stages I-IIIB. Predictors that patients would undergo max-LND were also evaluated.
Results: A total of 12,962 patients with gallbladder cancer were identified. We included 11,113 patients without distant metastases in our analysis. Multivariate analysis of Stage I-IIIB GBC demonstrated that strong predictors of improved survival are early tumor status, negative LNs and adjuvant treatments (p<0.001 for all). Predictors of worse overall survival are simple cholecystectomy (HR 1.74; p<0.001) and minimal LND (HR 2.56; p<0.001). When evaluated by tumor stage, the extent of LN removal did not significantly affect mean overall survival of Stage I GBC. In contrast, the extent of LND for GBC was significantly associated with improved overall survival of patients with Stage II (T2N0), Stage IIIA (T3N0) and Stage IIIB (T1-3,N1) disease (p<0.01 for all; see Table).
The likelihood that max-LND was performed was predicted by younger age (p<0.001), as well as T4 tumor status compared to T1-3 (p<.001). No LNs were recovered in 74%, 60% and 50% of patients with Stage I, II and III disease respectively.
Conclusions: This is the largest population-based study of patients with GBC in the literature. Not surprisingly, early tumor stage and adjuvant therapy correlate with survival. In addition we found radical cholecystectomy and maximal LND correlate with survival even in node negative patients (Stage II and IIIA). Our results support an approach of radical cholecystectomy and extensive LN dissection for Stage II and III disease, and also suggest that many patients in the US with GBC are currently surgically undertreated. These patients may not be receiving the best chance for control of an otherwise difficult disease. Finally, the finding that LND benefits patients with N0 disease raises questions about current methods of LN analysis.
Comparison of Survival by Stage and Extent of Lymph Node Dissection
| Stage | Minimal LND - OS | Maximal LND - OS | p value | | I | 50.5 mo | 58.2 mo | 0.196 | | II | 40.8 mo | 57.4 mo | <0.001 | | IIIA | 27.2 mo | 43.2 mo | 0.01 | | IIIB | 21.2 mo | 31.9 mo | <0.001 |
OS - Overall Survival, LND - Lymph Node dissection, mo - months.
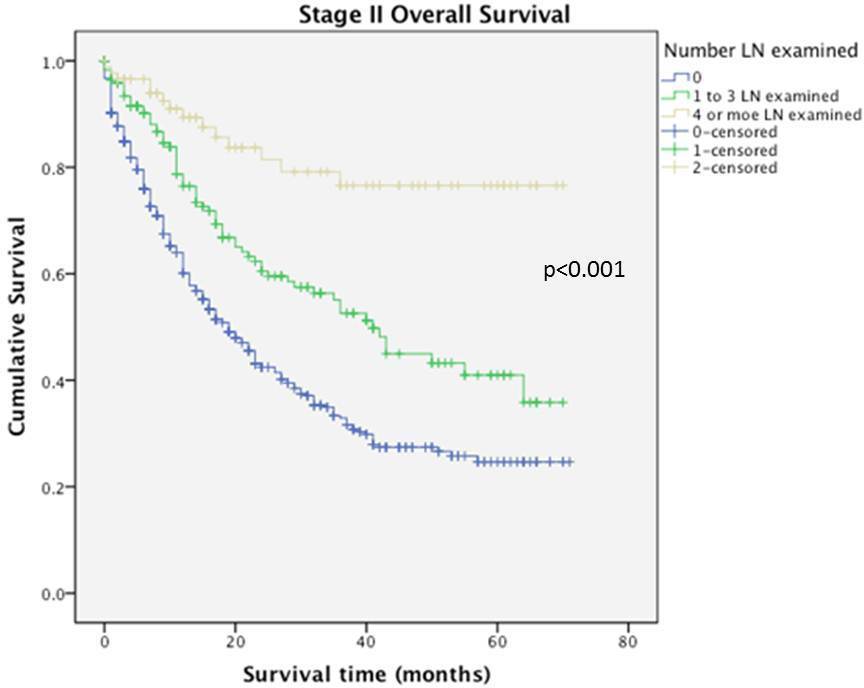
Overall Survival of Stage II Disease Related to Extent of Lymph Node Dissection
Back to Annual Meeting Program
|

