
Mirizzi syndrome is an atypical presentation of gallstone disease in which the impaction of a gallstone in either the cystic duct or the gallbladder causes stenosis of the extrahepatic bile duct by extrinsic compression and/or fibrosis. In some cases, the associated inflammation progresses to cholecystocholedochal fistula formation. The Mirizzi syndrome incidence is 0.7- 2.5% of all patients undergoing cholecystectomy. It is important to surgeons because the diagnosis may not be made preoperatively and it is associated with an increased risk of bile duct injury. Accurate definition of the biliary anatomy preoperatively is essential for optimal surgical planning.The present case describes Mirizzi syndrome classified as type IV in a 77 year-old man with abdominal pain without clinical jaundice, normal bilirubin level and an alkaline phosphatase slightly elevated. Abdominal ultrasound suggested dilated intrahepatic bile ducts and gallstones. Patient underwent endoscopic retrograde cholangiopancreatography (ERCP) which demonstrated a dilated extra and intrahepatic biliary tree compatible with a Klatskin tumor. Magnetic Resonance cholangiopancreatography (MRCP) also suggested a Cholangiocarcinoma at the common hepatic duct junction. Patient underwent an exploratory laparotomy with Mirizzi syndrome type IV being confirmed during cholecystectomy, with extraction of a 2.3 cm stone from the common bile duct. Roux-Y- HepaticoJejunostomy reconstruccion was performed as a final treatment for Mirizzi syndrome type IV. Mirizzi syndrome is rarely diagnosed preoperatively and it remains a diagnostic and therapeutic challenge for endoscopists and biliary surgeons.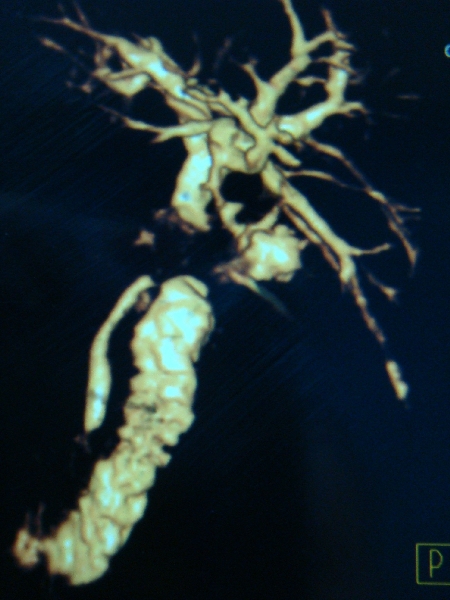
MRCP: Defect at CHD junction
 500 Cummings Center
500 Cummings Center +1 978-927-8330
+1 978-927-8330
 +1 978-524-0461
+1 978-524-0461
