
Objective: To determine the prognostic significance of the number of positive nodes in patients with node positive pancreas cancer.
Methods: SEER data(1988-2002) was used to identify 4939 patients who underwent pancreatic resection for adenocarcinoma, including 2116 patients pathologically staged as node positive. The number of positive lymph nodes was redefined as a dichotomous variable called positive lymph node cut point (pLNCP) ranging from 1-6. Survival analysis was performed on the node positive cohort using an overall survival endpoint. Multivariate model variables included age, sex, T-stage, grade, radiation therapy and number of positive lymph nodes.
Results: Univariate survival analysis of pLNCP's 1-6 by log rank test demonstrated that >4 positive lymph nodes resulted in the statistically strongest difference in survival within the node positive cohort (χ2statistic=25). Kaplan-Meier survival curves based on pLNCP=4 demonstrated a decrease in median survival difference of 3 months (p<0.001) for patients found to have >4 positive nodes compared to patients with <4 positive nodes. Multivariate analysis validated having >4 positive lymph nodes was a strong independent predictor of death (HR=1.23, 95%CI 1.1-1.4, p<0.001).
Conclusion: Resected node-positive adenocarcinoma of the pancreas is considered Stage IIB regardless of the number of positive nodes. This study has shown that a patient having >4 positive nodes is 24% more likely to experience death and has an associated decrease in median survival of 3 months compared to patients with <4 positive nodes. Given this significant and relatively large survival difference in the setting of such an aggressive biology, we have defined N2 disease as >4 positive nodes. Evaluation of future trials may benefit from utilizing N2 disease in stratification schema.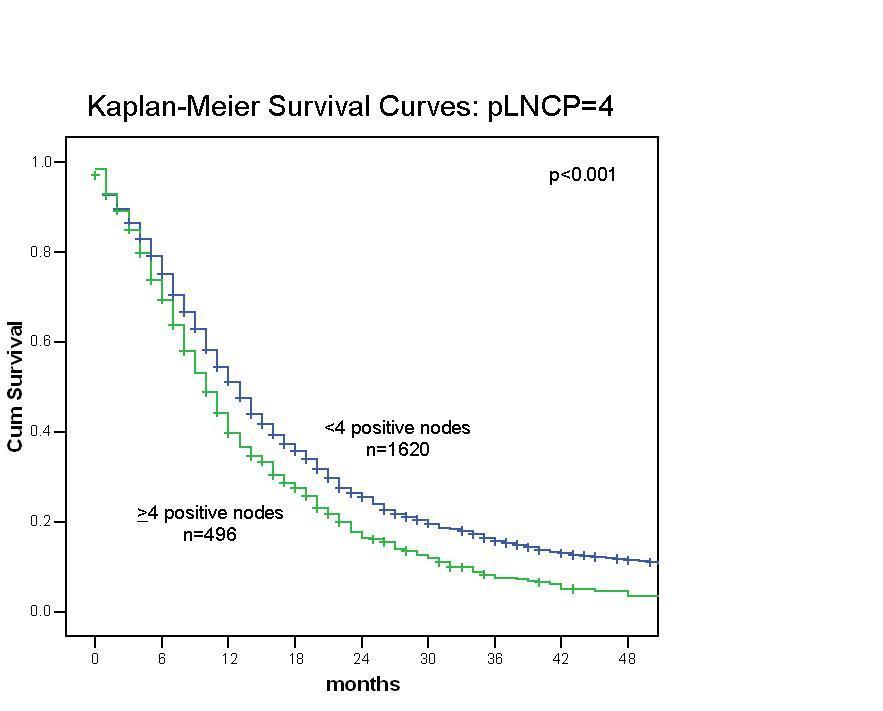
 500 Cummings Center
500 Cummings Center +1 978-927-8330
+1 978-927-8330
 +1 978-524-0461
+1 978-524-0461
