
Objective:
Successful anastomosis is crucial for success of esophagogastrectomy (EG). Before July 2002 almost all esophagogastric anastomoses at our institution were hand-sewn (HSA). We then began utilizing a linear stapled anastomotic technique (LSA). This review compares the outcomes of patients with HSA and LSA following EG.
Methods:
Two-hundred eighty consecutive patients with EG and gastric reconstruction from July 2001 to June 2004 were reviewed.
Results:
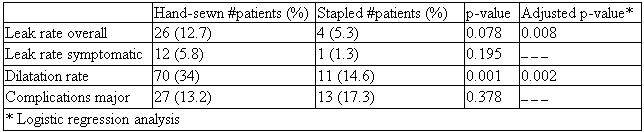
There were 235 men, 45 women. Median age: 65 years (range 22 - 95 years). Indications were malignancy in 244 patients, high-grade dysplasia in 22, benign conditions in 14. Ivor Lewis EG was performed in 196 patients (70%), transhiatal 70 (25%), left thoracoabdominal 10 (4%), and extended esophagectomy in 4 (1%). Anastomosis was intrathoracic in 206 patients (74%) and cervical in 74. HSAs was performed in 205 patients (73%) and LSAs in 75 (27%). LSA was intrathoracic in 33 patients (16%) and cervical in 42 (57%). One-hundred seventeen patients (42%) received neoadjuvant therapy. Five patients died (mortality, 1.8%). Anastomotic leaks occurred in 30 patients (11%): cervical in 11 (15.1%) and intrathoracic in 19 (9.2%) (p=0.013). Leaks were asymptomatic in 17 patients (57%). Thirteen patients (4.6%) had symptomatic leaks requiring re-operation. Other major complications occurred in 40 patients (14.3%). Median hospitalization: 10 days (range 6 - 98 days). Median follow-up: 9 months (range 0.25 - 38 months). Overall, 81 patients required dilatation (median 2; range 1 to 14); 70 (34%) had HSA and 11 (14.6%) LSA (p=0.001). HSAs were more likely to leak and require dilatation; odds ratios and 95% confidence intervals were 5.35 (1.67-19.27) and 3.58 (1.66-8.34) respectively.
Conclusions:
A linear stapled esophagogastric anastomosis (LSA) is safe and associated with significantly lower leak rate and need for dilatation than hand-sewn anastomosis (HSA). This non-randomized series suggests that LSA is the preferred anastomotic technique regardless of surgical approach.
Comparison of Hand-sewn and Linear stapled anastomoses
 500 Cummings Center
500 Cummings Center +1 978-927-8330
+1 978-927-8330
 +1 978-524-0461
+1 978-524-0461
